Overview
Eicosapentaenoic acid (EPA) is a long-chain omega-3 fatty acid primarily found in marine sources that plays a key role in cardiovascular and inflammatory regulation. EPA exerts cardioprotective effects through multiple mechanisms, including triglyceride reduction, anti-inflammatory actions, improved endothelial function, and stabilization of atherosclerotic plaques. Evidence from randomized controlled trials and meta-analyses indicates that EPA supplementation, particularly at higher doses (≥1 g/day), is associated with a significant reduction in major adverse cardiovascular events (MACE), especially in individuals with elevated triglycerides or established cardiovascular disease. A dose-related meta-analysis found that omega-3 supplementation providing at least 1 g/day of EPA (alone or with DHA) reduced myocardial infarction risk by 14–19% [6]. In the VITAL trial, supplementation with 460 mg/day EPA + 380 mg/day DHA increased circulating lipid mediators of inflammation resolution, particularly in individuals with low baseline fish intake [4]. Earlier trials also support cardiovascular benefits of marine n-3 fatty acids post-myocardial infarction, though recent studies show more modest effects in populations already receiving optimal medical therapy [1][2].
Dosage Guide
Recommended Daily Allowance
For generally healthy individuals
Therapeutic Doses
For treatment of specific conditions
Upper Intake Limit
Maximum safe daily intake
5000 mg— FDA considers up to 5 g/day of EPA+DHA from supplements as generally safe
Special Forms
Alternative forms for specific needs
Prescription-only, high-purity EPA; proven cardiovascular benefit in high-risk patients
Triglyceride form may have better bioavailability, especially with low-fat meals
Clinical Notes
- High-dose EPA may increase bleeding risk, especially when combined with anticoagulants; monitor in surgical settings
- Prescription EPA (e.g., icosapent ethyl) has demonstrated cardiovascular benefit independent of triglyceride-lowering [6]
- Omega-3 supplements may slightly increase LDL cholesterol in some individuals; monitor lipid panels
- Effectiveness may be greater in individuals with low baseline fish intake or elevated triglycerides
- Ensure product purity: choose third-party tested supplements to avoid contaminants (e.g., mercury, PCBs)
Research
Marine n-3 fatty acids (EPA and DHA) showed protective trends against cardiovascular events in post-MI patients on modern therapy.
Omega-3 supplementation may have modest benefits for cardiovascular prevention, with stronger evidence for secondary prevention.
Omega-3 fatty acids show potential but inconsistent effects on cardiovascular outcomes in primary and secondary prevention.
Supplementation with 460 mg EPA + 380 mg DHA/day increased pro-resolving lipid mediators, especially in low fish consumers.
Omega-3 fatty acids may reduce cardiovascular risk, with stronger effects in high-risk populations.
Dose-response analysis showed significant reduction in myocardial infarction with ≥1 g/day omega-3 supplementation.
EPA incorporates into cell membranes in a dose- and time-dependent manner, with effects plateauing after several weeks.
Plasma phosphatidylcholine EPA levels increase dose-dependently with fish oil supplementation, confirming biomarker sensitivity.
Products Containing EPA(2 reports)
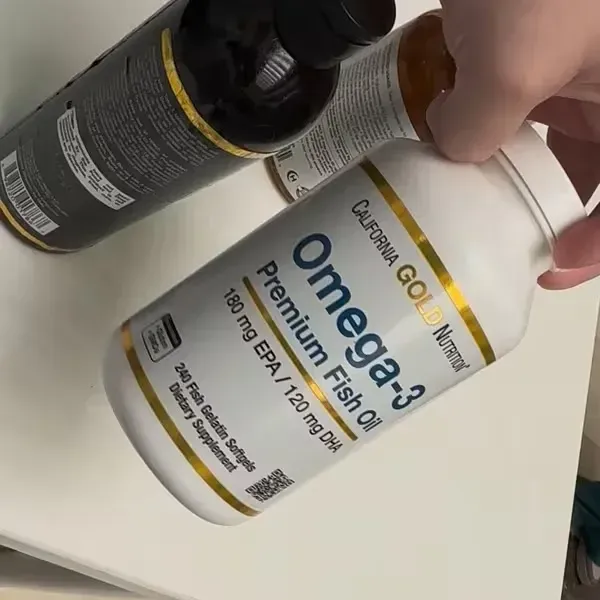
Omega-3 Premium Fish Oil by California Gold Nutrition provides 180 mg of EPA and 120 mg of DHA per serving, derived from fish oil. These omega-3 fatty acids support cardiovascular and cognitive health and contribute to the resolution of inflammation. The formulation aligns with typical over-the-counter supplement profiles, though higher doses may be needed for specific clinical outcomes.
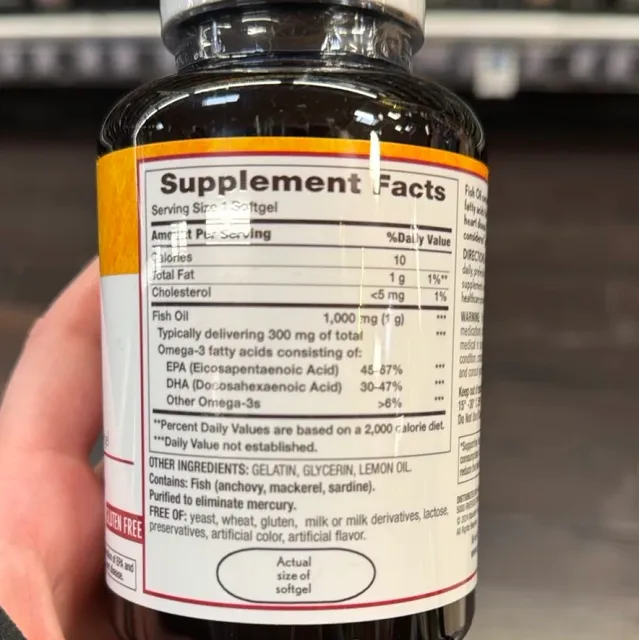
This over-the-counter fish oil supplement provides 300 mg of combined EPA and DHA per softgel, falling below the clinical dose range for cardiovascular or mental health benefits. While it delivers a modest amount of omega-3 fatty acids, higher-dose, prescription-grade formulations have demonstrated more consistent therapeutic effects in high-risk populations.